There are several recommendations on the opportunities when health-care workers (HCW) should perform hand hygiene. Perhaps the most widely known guideline is the ‘My 5 Moments for Hand Hygiene’ developed by the WHO.
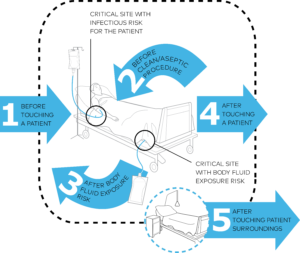
WHO ‘My 5 Moments for Hand Hygiene’
Modifications of the WHO 5 moments protocol also exist, like the Canadian Ontario Ministry recommendations called ‘Your 4 Moments for Hand Hygiene’. CDC also has similar indications.
WHO claims that these 5 moments present the highest risk for pathogen transmission [1]. According to Kelly 2015, moments #2 and #3 (M2 and M3) are the highest risk moments [2]. Bingham 2016 examined thoroughly the contamination of healthcare workers hand before M2 and after M3. In both cases, 17% of HCW acquired at least one type of pathogen on their hands. This finding proves the special importance of these moments [3].
Several studies focus on the HCWs’ compliance to the WHO 5 moments protocol:
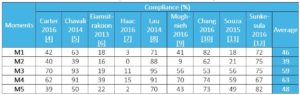
Sources: Carter 2016 [4], Chavali 2014 [5], Eiamsit-rakoon 2013 [6], Haac 2016 [7], Lau 2014 [8], Moghnieh 2016 [9], Chang 2016 [10], Souza 2015 [11], Sunkesula 2016 [12]
As the data shows, compliance values are highly variable among hospitals, and probably depend on the experiment settings (e.g., direct or video observation was applied). Depending on the observation method employed in the study, the significant distorting of the Hawthorne effect should also be considered (see on this issue our upcoming post). On average, lowest compliance was observed before aseptic procedure (M2). This can be explained by gloves use (which issue will be covered separately on this blog); in Haac 2016 before M2 no healthcare worker performed hand hygiene although they donned new gloves 75% of the time. Moghnieh 2016 had the same conclusion, and they suggest HCWs should be educated that gloves do not prevent cross-infections in the absence of hand hygiene before wearing them. Highest compliance was observed after touching patient and exposure to body fluid (M3 and M4). According to Chavali 2014, this reflects an urge to HCW protect themselves.
Conclusion:
There are clear recommendations when should a healthcare worker perform hand hygiene. The necessary of these steps are verified by microbiological results. Yet, compliance needs to be improved. Our technology is aimed to support HCWs in the most critical moments, and provide assurance on hand hygiene when it’s most needed. Semmelweis Scanner can thus be placed e.g., at a central location in an ICU, where all HCWs can easily get access to it.
Ream more on Electronic Compliance Monitoring Systems