Last time we wrote about the current 6-step hand hygiene protocol, which formed the base of the EN1500 and WHO hand hygiene recommendations.
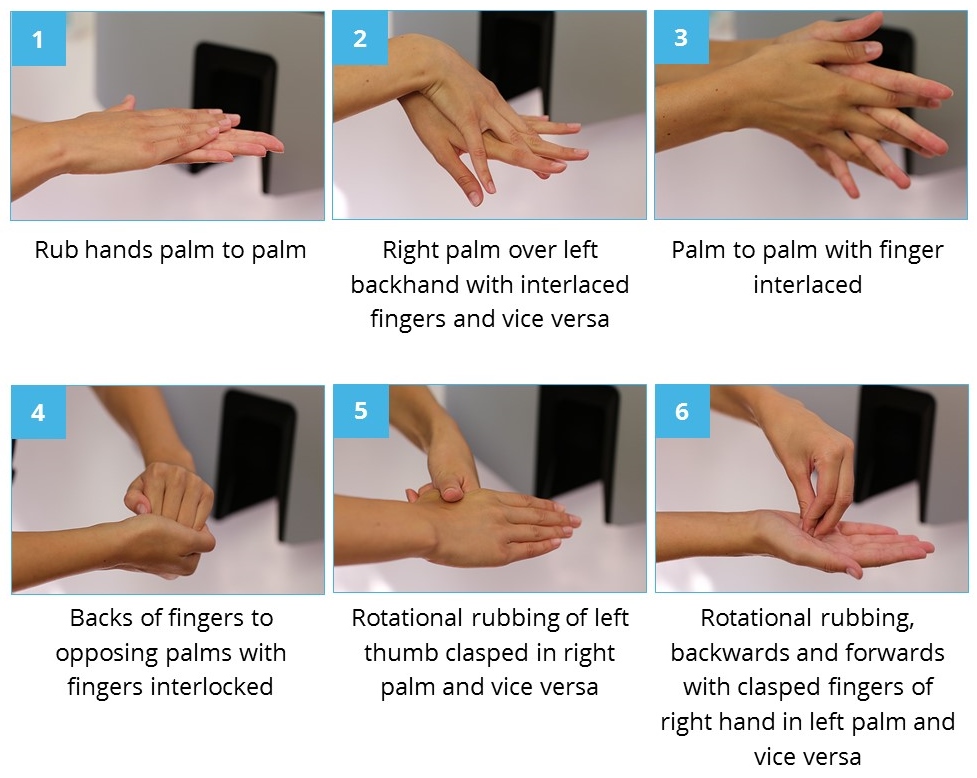
Figure 1: The 6-step from WHO ‘How to handrub’ and ‘How to handwash’ guide [1].
There are two problems with the 6-step protocol, that are often reported. First, it takes too long to perform. Kampf 2008 reported that performing the 6-steps protocol accurately lasts on average 75 s, while the guideline only requires 30 s.
Second, according to several studies, 6 steps are too many to remember. In Silva 2014, healthcare professionals were asked about hand hygiene; 98.6% of them replied that they feel very motivated to perform hand hygiene, yet, 38% failed to report the steps of the hand washing technique adequately. Arias 2015 evaluated the compliance of the 6-step by direct observation, and found that while the first two step’s compliance was 100%, thumbs (step5) and fingertips (step6) were achieved only in 15% and 37% of the cases. Squeri 2016 described that in 71% of the cases healthcare workers did not follow neither the timing nor the method suggested by the WHO guidelines.
Tschudin-Sutter 2016 suggests a simplification of the WHO 6-step protocol; the new protocol only contains step1, step5 and step6 of the original protocol. They found that the compliance to the simplified protocol was 54%, while the compliance to the original protocol was only 16%. In lights of this, it is not surprising that microbiological analyses revealed no significant differences in bacterial counts. They suggest that the conventional 6-step could be safely replaced by a simpler hand hygiene technique. This idea is now under more thorough investigation.
Kampf 2008 investigated 16 variations of hand hygiene steps. Based on their research, they proposed a new, 5-step protocol, where every step repeated only twice.
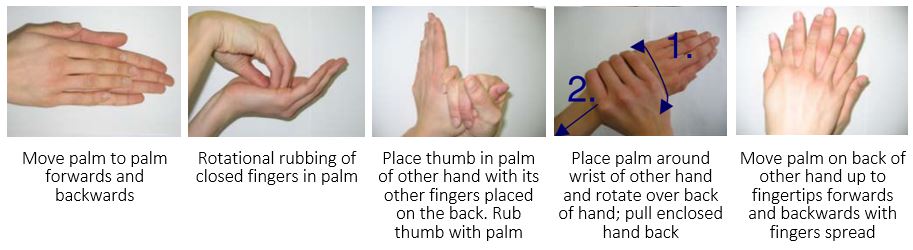
Figure 2: A 5-step protocol suggested by Kampf 2008
Kampf 2008 has other interesting findings; they noticed quite good performance among non-healthcare volunteers. They explained it by the repeated feedback given on their individual performance. Based on this, they claimed that strict, stepwise protocol is not necessary; the promotion of “responsible application” (allowing the individual to use his or her own procedure) combined with individual training may be an appropriate way to ensure high quality in hand disinfection.
In Haidegger 2016, coverage of hand with alcoholic handrub were investigated by the means of the Semmelweis Scanner. This device gives visual objective feedback on the coverage immediately after the hand hygiene event. At the first time, only 58% of the examined healthcare workers reached complete coverage. Continuously monitoring and feedback lead to a significant improvement; for the 5th measurement 87% reached complete coverage.
Conclusion:
6-step guide for hand hygiene is a really useful starting point, however we need to keep in mind that the goal is not the compliance to the protocol, but the complete coverage of hands, regardless of the method applied. To reach complete coverage, personal feedback about the hand hygiene performance is essential.