What is the difference?
If we are about to find a proper alcohol-based hand hygiene product, we can select from a broad spectrum; liquid format hand sanitizers (rinses), gels and foams are available across a wide spectrum. But which one is the best, and what factors should we consider when choosing?
Rinses were the first alcohol-based hand disinfectant products. They were not skin-friendly, caused skin irritation and dryness for many healthcare workers (HCW). That is why gels and foams were developed. In 2002, Kramer et al. compared several hand gels and rinses. They concluded that rinses have significantly greater bacterial reduction factor than gels. Gels available in those days did not meet the EN 1500 standard, so they are not suitable for health-care settings [1].
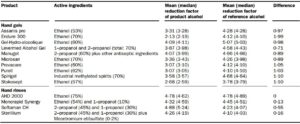 Figure 1: Efficacy of alcohol-based hand hygiene products, and the EN 1500 reference alcohol,
Figure 1: Efficacy of alcohol-based hand hygiene products, and the EN 1500 reference alcohol,
60% propan-2-ol (Source: Kramer et al. 2012)
The conclusion of this study was quite controversial; many groups around the world expressed criticism. Hoffmann et al. argued that gel can kill 99.9% of contamination sources. It’s an order of magnitude less, of what rinses can reach, but may be enough during routine work. They believed that any factor making a product more acceptable to users is as important as an order of magnitude difference in efficacy. If HCW do not like to use a product, compliance will decline. User acceptance is vital to the overall effectiveness [2]. Diekema D. argued that the correlation between test condition data of bacterial reduction and the risk for pathogen transmission is unclear. On the other hand, HCW’s skin health is an important issue [3]. According to Girard et al., good adherence is only possible if the product is well tolerated. They reported that when they changed from rinse to gel, the number of handrubbing events have doubled [4].
The need of better gels and foams were clear. Sterillium Gel were introduced at that time, as the first gel containing as high as 85% ethanol, and it was probably the first gel to pass EN 1500 in 30 seconds [5]. Barbut et al. compared the reduction factor of Sterillium gel and Sterillium rinse, and they did not find a difference (1.29±0.84 and 1.28±0.95 log(10) CFU/mL). In the same study, overall compliance raised at places where the gel was available. They advised, if products have a similar antimicrobial activity, the choice should take into account the HCW’s acceptance [6].
In 2012 Edmonds et al. investigated several commercially available products and also the WHO recommended formulations. They concluded that simply including alcohol at a concentration >75% will not guarantee that an ABHR formulation will meet global efficacy standards, because other ingredients may significantly influence the antimicrobial properties. Alcohol concentration alone cannot guarantee the quality of a product [7].
In 2014 Macinga et al. focused on another problem; some products dry too slowly, thereby encouraging the use of inadequate volumes. All investigated products met EN 1500 with 3 ml volume and 30 seconds, but this 3 ml takes longer than 30 seconds to dry. They found that delivery format do not really influence the drying time, but alcohol concentration does. They also found that rinses drip from the hands more often; in the case of gels and foams, there is a higher chance that the entire volume remains on the hands [8].

Figure 2: Mean dry-time of different products and frequency of dripping out. (Foam B – Purell Advanced Foam, Gel C – Purell Advanced Gel, Rinse D – Experimental prototype) (Source: Macinga et al. 2014)
Products still need improvement in some areas. In 2012, Prado at al. compared the antimicrobial efficacy of 12 alcohol-based hand gels produced in Brazil. 10 out of 12 met EN 1500 with 60 seconds, and only 4 met EN 1500 with 30 seconds’ application time [9].
Larson et al. investigated the virucidal effect of different forms of hand hygiene products (foam – Alcare, Steris, gel – Purell, GOJO and a hand wipe) in 2012, and found no difference [10].
Kaiser et al. reported that some alcohol-based products can react with chlorhexidine gluconate (CHG). CHG is a disinfectant and antiseptic that is used for skin disinfection before surgery. A well-known benefit of the use of CHG products that they have long-lasting disinfection effect on the skin. CHG persistent activity is based on its cationic character. The two most commonly used thickeners for handrub gels are both anionic polymer systems, and they can inactivate the effect of the CHG [11].
 Figure 3: Inactivation of CHG persistence by alcohol-based hand hygiene products. (Source: Kaiser et al. 2009)
Figure 3: Inactivation of CHG persistence by alcohol-based hand hygiene products. (Source: Kaiser et al. 2009)
Conclusion:
Alcohol-based hand hygiene products are available in several delivery formats; rinses, gels and foams. They can be compared along many parameters; gels and foams are typically more skin friendly, and will drip out less frequently. Rinses has higher antimicrobial effect, but some modern gels and foams are as effective as the rinses. If the use of chlorhexidine gluconate products is part of the daily routine, we need to pay attention to product compatibility. And finally, one of the most important parts; product acceptance is a major factor in compliance. Before you select a product, ask your team what they prefer!
Read our previous post on the composition of handrubs. Please stand by for our next blog entry on the skin irritation of the hand hygiene products.