The Hawthorne effect is a well-described psychological phenomenon, it basically means that people (and even animals) change their behavior if they know that they are being observed by someone. As the direct observation is the gold standard for monitoring hand hygiene compliance, we need to better understand the influence of the Hawthorne effect [1].
The Hawthorne effect was first reported in the 1950s, at Western Electric telephone manufacturing factory at Hawthorne (near Chicago), where they carried out a study about how the modification of environmental factors (lighting, temperature, work hours, etc.) can change productivity [2]. They got a quite surprising result; “no matter what factors they manipulated, productivity went up. Even when work conditions were made worse than they were originally, the personnel worked harder and more efficiently.” They concluded that the rise in productivity was only because the workers knew they were observed [3].
The Hawthorne effect has a huge impact on hand hygiene compliance monitoring. Healthcare-workers (HCW) try to meet the observer’s expectations, especially when they know that IPC is being pushed as an institutional priority. It is not necessarily cheating from the HCW’s point of view, it is more a social desirability bias. Also, the observer itself can serve as a reminder not to forget about hand hygiene [3].
 Figure 1.: Hand hygiene training.
Figure 1.: Hand hygiene training.
How can we measure the Hawthorne effect?
Kovacs-Litman et al. 2016 tried to quantify the Hawthorne effect in IPC. Two students covertly measured hand hygiene compliance, and they compared the data to the result of the open observation. They found that hand hygiene compliance was 50.0% during covert observation and 83.7% when hospital auditors measured it overtly. They concluded that traditional hand hygiene audits can overestimate hand hygiene performance [4].
A quite similar experiment was carried out at the National Taiwan University Hospital by Pan et al. 2013. They also used medical students as covert observers. Overt observation consisted infection control nurses and hand hygiene ambassadors, who were responsible for hand hygiene education, communication and feedback. Annual compliance rates were reported at 44.1% by the covert students, while 74.4% was reported by infection control nurses, and 94.1% reported by the hand hygiene ambassadors [5].
Eckmanns et al. 2006 monitored the hand hygiene compliance during two different periods. At first, HCW had no knowledge of being observed. During this period, the overall compliance rate was 29%. At the second period, they announced to HCW that observers would be monitoring the hand hygiene compliance. During this second period compliance went up to 45% [6].
Srigley et al. 2014 designed a study in an academic acute care hospital, where the hand hygiene product usage was continuously monitored by a real-time location system (RTLS) over an 8-month-long period. When hand hygiene auditors arrived to the unit, their movements were also tracked by the RTLS. They found that hand hygiene event rate was 3.75/dispenser/hour at dispensers that were
visible to auditors, while at the same time, in the case of dispensers that were not in sight of the auditors, this number was only 1.48/dispenser/hour. They had also examined the same dispenser’s weekly usage beforehand, and found 1.07/dispenser/hour value. Hand hygiene rates were approximately threefold higher within the eyesight of an auditor [7].
Hagel et. al. 2015 also used electronic systems combined with direct human observation. 70 electronic hand hygiene dispensers were installed in the ICU, that continuously recorded hand hygiene events. Direct observation was performed by a medical student. They compared the dispenser usage data and observed a significant increase, from 8 hand hygiene events/hour without direct observation to 21 hand hygiene events/hour during direct observation [8].
According the Chen et al. 2015, the Hawthorne effect is time-dependent; the magnitude of the effect depends on how long the participant are aware of the observation.
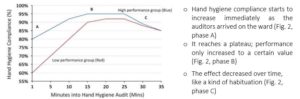
Figure 2.: Time-dependent change in hand hygiene compliance. (Source: Chen et al. 2015)
Some studies claim that electronic hand hygiene monitoring systems (like RFID tags, sensors, video recorder, etc.) generate less intense Hawthorne effect than direct human observation, but do not eliminate it [3].
The Hawthorne effect is usually described as a factor that needs to be eliminated, because it modifies the compliance results. But we can also utilize the Hawthorne effect, like when police cars are used on the roads to reduce speeding. When people notice that they are under observation, they start to behave different – better [3]. The only thing we need to keep in mind is that the Hawthorne effect does not takes any longer than the period of time whilst subjects know they are under observation. If we want to take advantage of this effect, we need to apply continuous monitoring, although the effect decrease over time.
Conclusion:
It is important to recognize that the Hawthorne effect exists, and keep in mind while we design a study, or in the process of analyzing compliance data. If our institution’s data is “too good to be true” than we should take into consideration that we might have recorded the Hawthorne effect [1]. Electronic monitoring system can help to reduce the Hawthorne effect, and continuous monitoring can have positive effect to HCW behavior.
Read our previous post about when should we perform hand hygiene. Please stand by for our next blog entry on the objectivity of direct observation.